Rationale.
Modern needs and requirements of patients for full restoration of aesthetics and function of the dentition system encourage doctors to use not only conservative methods, but also a whole range of surgical interventions during preparation for orthodontic and orthopedic treatment [4, 6]. It is precisely the control of regeneration processes that allows for predictable, high-quality treatment results and reduces the risk of possible early and late complications thanks to the desired course of the wound healing process and scar formation [6, 8]. A high percentage of patients with affected periodontal complex receive combined treatment, where surgical interventions are the mainstay. Operations performed in the areas of the mucogingival junction and fixed gums have a large postoperative wound surface that requires careful antiseptic care throughout the entire wound healing process until complete healing and control over scar tissue formation [8].
Wound surfaces in the oral cavity are constantly in contact with oral fluids, food, etc., which leads to trauma and infection of postoperative areas [7]. This prompts the search for and use of protective materials for wound areas in the postoperative period that would help protect the adjacent healthy gums and completely close the wounds formed during surgical intervention for frenuloplasty, frenuloplasty, vestibuloplasty, and recession closure, protect the marginal periodontium, and promote the adaptation and restoration of soft tissues, covering the suture lines in the areas of postoperative interventions [14].
The aim of the study. Improving the effectiveness of comprehensive treatment and prevention of possible complications after surgical intervention on the oral mucosa by using the “Ora-Aid” polymer protective membrane and “Kvertgial” mucoadhesive gel.
Object and methods of research. The control and main groups consisted of 68 patients, 34 in each, who had indications for surgical intervention due to abnormal attachment of the soft tissues of the vestibule of the oral cavity and recession of the gingival margin.
Surgical interventions were performed in the areas of the mucogingival junction and fixed gums. The large wound surfaces formed during the surgical interventions required careful antiseptic care throughout the healing period.
The control group of patients received a standard set of therapeutic measures, which consisted of professional oral hygiene, removal of supragingival and subgingival deposits if necessary, replacement of irrational fillings and prostheses, elimination of traumatic occlusion points, and local drug therapy.
In the main group of patients, in addition to the standard set of therapeutic measures, the “Ora-Aid” polymer protective membrane (TBM Corp., Korea) and the “Kvertgial” mucoadhesive gel (“Odessa Biotechnology,” Ukraine) were used.
The gel was applied after surgical interventions, over the wound, to stimulate regeneration processes, after which the wound surface was covered with a protective membrane. The technique used helps to create a depot of the active substance in the area of surgical intervention and allows for increased treatment effectiveness. The course of treatment is twice a day for 14 days. “Ora-Aid” adheres firmly to the wound surfaces in the oral cavity and slowly dissolves on its own. The affected area is hermetically isolated from the environment, which prevents secondary infection of the wound, ensures active and selective action of the therapeutic factor on the affected area, and controls the release of therapeutic ingredients from the dressing into the oral cavity and the entry of microorganisms into the area of gel action.
Biochemical studies of the oral fluid of the patients under observation were conducted at the initial stage, after 3 days (following surgical intervention according to the protocol and the prescription of a therapeutic and prophylactic complex (TPC)), 7 days after treatment, 14 days, and 6 months after surgical treatment. The activity of urease, which indicates the level of contamination of the oral cavity with opportunistic and pathogenic microbiota [2], and the activity of lysozyme, which reflects nonspecific antimicrobial protection.
Results and discussion.
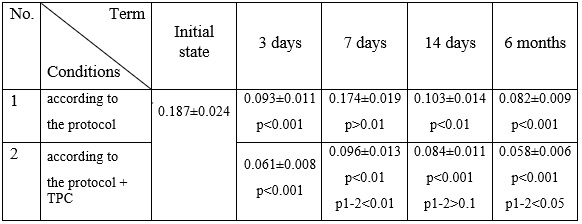
Urease is not produced by somatic cells and probiotic bacteria, but is secreted by opportunistic and pathogenic microbiota, in particular Klebsiella oxytoca, Morganella morganii, Proteus mirabilis, Providencia stuartii, Providencia rettgeri, Problecia etjereiu, Klebsiella pneumoniae. The level of urease in oral fluid may indirectly reflect the degree of colonization of the oral cavity by opportunistic microbiota. The results of this study are presented in Table 1. As can be seen from the data presented, urease activity in the oral fluid of patients at the initial stage of the study was very high – 0.187 μkat/L (normal range 0.040-0.080 μkat/L).
Table 1
Dynamics of changes in urease activity in the oral fluid of patients after surgical intervention and various treatment regimens, mk-kat/l
Analysis of the oral fluid of patients observed 3 days after standard treatment and/or prescription of TPC showed a significant decrease in urease activity in all groups, but to varying degrees. Thus, in the oral fluid of the 1st group, this indicator decreased by 2.0 times, and in the 2nd group by 3.1 times compared to the initial level. The results obtained indicate the ability of TPC to significantly reduce bacterial contamination of the oral cavity (Table 1).
Analysis of the oral fluid of the patients observed 7 days after various treatment regimens showed an increase in urease activity in the first group to the initial level (p > 0.1). In the oral fluid of the second group, urease activity remained at a significantly low level relative to the initial state value (p<0.001-0.05).
Research conducted 14 days later showed low levels of urease activity in the oral fluid of all groups (p < 0.01 - 0.001). These data indicate the effectiveness of antimicrobial therapy and the use of subsequent treatment regimens with a clear advantage of prescribing TPC.
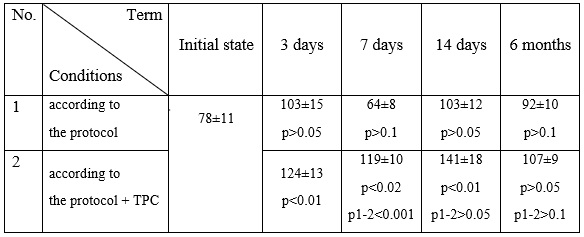
The results of the analysis of patients' oral fluid for the content of this nonspecific antimicrobial factor in the oral cavity are presented in Table 3. Initial examination of oral fluid showed low lysozyme activity in the oral fluid of patients in the postoperative period. These results indicate an insufficient level of nonspecific antimicrobial protection in the oral cavity, which may explain the high urease activity in the oral fluid of patients.
On the third day after the surgical intervention and additional prescription of the therapeutic and prophylactic complex, a secondary analysis of the oral fluid of the patients under observation was performed. It was found that after oral cavity sanitation in group 1, lysozyme activity did not undergo significant changes (p > 0.05). Meanwhile, in the oral fluid of patients who additionally received the therapeutic and prophylactic complex, the studied indicator increased by 1.6 times (p<0.01, Table 3).
At the next stage of the study, 7 days after surgery, high lysozyme activity was found in the oral fluid of patients in group 2. The level of lysozyme activity in the oral fluid of patients in this group significantly exceeded the initial values (p<0.002 - 0.01). In the oral fluid of patients in group 1, who were treated according to the protocol followed by surgical treatment, lysozyme activity decreased to its initial level after 17 days (p >0.1).
Table 2
Dynamics of changes in lysozyme activity in the oral fluid of patients after surgical intervention and various treatment regimens, U/L
An analysis of oral fluid conducted 14 days after treatment showed high levels of lysozyme activity in group 2, exceeding initial values by 1.7-1.8 times.
Thus, the results in Table 2 indicate stimulation of the production of the antimicrobial factor lysozyme in the oral cavity of patients under the influence of the therapeutic and prophylactic complex.
Conclusions. Conducted biochemical studies of oral fluid have proven that the most effective method of preventing postoperative complications and accelerating healing is the prescription of the proposed TPC. The studied markers of inflammation and the degree of bacterial contamination decreased the most against the background of normalization of nonspecific resistance parameters. The changes observed were stable, as they persisted throughout the observation period. The most likely leading mechanism for normalizing homeostasis in the oral cavity of patients is the stimulation of the antimicrobial and antioxidant systems by TPC components, which prevented the activation of inflammation, the flare-up of LPO, and bacterial proliferation caused by surgical treatment.
References:
1. Døving, M., Handal, T., & Galteland, P. (2020). Bacterial odontogenic infections. Tidsskr Nor Laegeforen. 140(7). English, Norwegian. DOI: 10.4045/tidsskr.19.0778.
2. Ferraboschi, P., Ciceri, S., & Grisenti P. (2021). Applications of Lysozyme, an Innate Immune Defense Factor, as an Alternative Antibiotic. Antibiotics, 10(12), 1534. DOI: 10.3390/antibiotics10121534
3. Hadwan, M.H., Hussein, M.J., Mohammed, R.M., Hadwan, A.M., Saad, Al-Kawaz, H., Al-Obaidy, S.S.M., & Al Talebi, Z.A. (2024). An improved method for measuring catalase activity in biological samples. Biol Methods Protoc, 9(1), bpae015. DOI: 10.1093/biomethods/bpae015.
4. Dunnill, C., Patton, T., Brennan, J., Barrett, J., Dryden, M., Cooke, J., Leaper, D., & Georgopoulos, N.T. (2017). Reactive oxygen species (ROS) and wound healing: the functional role of ROS and emerging ROS-modulating technologies for augmentation of the healing process. Int Wound J, 14(1), 89-96. DOI: 10.1111/iwj.12557.
5. Akaike, T. (2001). Role of free radicals in viral pathogenesis and mutation. Rev Med Virol, 11(2), 87-101. DOI: 10.1002/rmv.303.
6. Yaghobee, S., Rouzmeh, N., Aslroosta, H., Mahmoodi, S., Khorsand, A., & Kharrazifard, M.J. (2018). Effect of Topical Erythropoietin (EPO) on palatal wound healing subsequent to Free Gingival Grafting (FGG). Braz Oral Res, 32, e55. DOI: 10.1590/1807-3107bor-2018.vol32.0055.
7. Thoma, D.S., Naenni, N., Figuero, E., Hämmerle, C.H.F., Schwarz, F., Jung, R.E., & Sanz-Sánchez, I. (2018). Effects of soft tissue augmentation procedures on peri-implant health or disease: A systematic review and meta-analysis. Clin Oral Implants Res, 29(15), 32-49. DOI: 10.1111/clr.13114.
8. Zucchelli, G., Tavelli, L., McGuire, M.K., Rasperini, G., Feinberg, S.E., Wang, H.L., & Giannobile, W.V. (2020). Autogenous soft tissue grafting for periodontal and peri-implant plastic surgical reconstruction. J Periodontol, 91(1), 9-16. DOI: 10.1002/JPER.19-0350.
|